
Tameside and Glossop Integrated Care
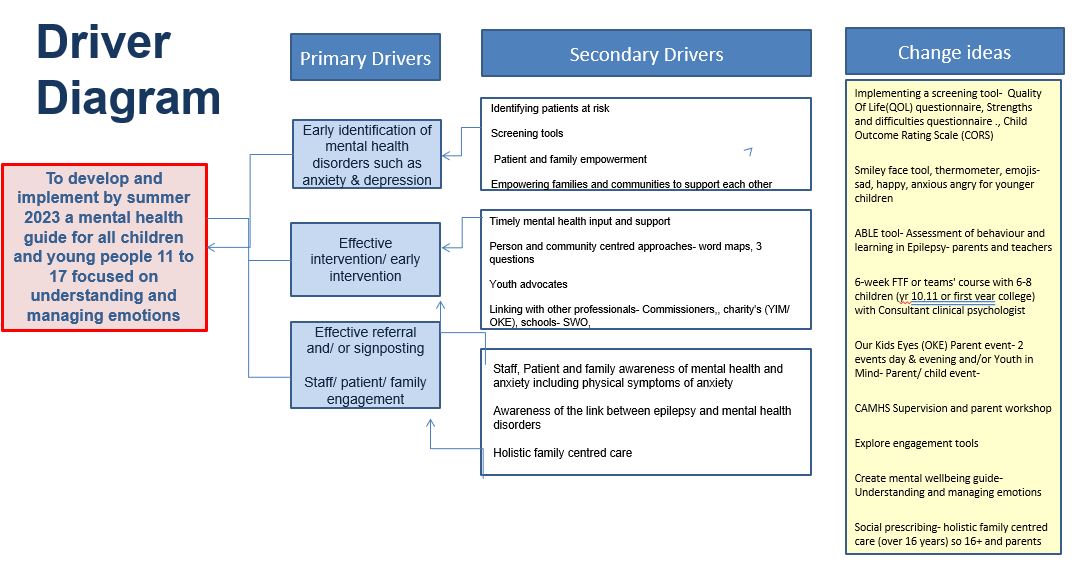
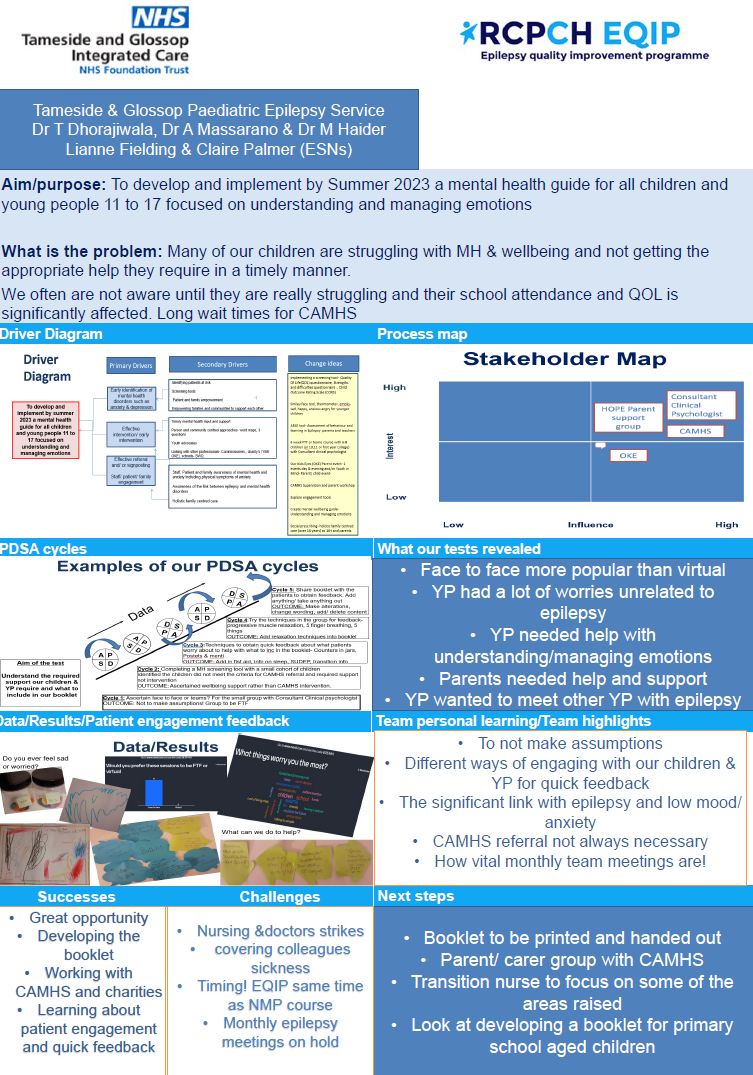
To develop and implement by Summer 2023 a mental health guide for all children and young people 11 to 17 focused on understanding and managing emotions.

Project aim
To develop and implement by Summer 2023 a mental health guide for all children and young people 11 to 17 focused on understanding and managing emotions.
Background
We provide a paediatric epilepsy service for children in Tameside and Glossop. In our team we have 2 paediatricians with an epilepsy interest, 1 paediatric neurologist (visiting) and 1 epilepsy nurse specialist. We have excellent links with tertiary neurologist who does 1 clinic a month and we regular discuss cases on an ad hoc basis. We have recently recruited a further paediatrician and are in the process of recruiting a transition nurse specialist (initial funding by Roald Dahl). We have around 200-250 patients on our case load at any one time. We have community links with our special needs schools and allied health professions (HV, physion, OT, SALT, dieticians).
We are continuous undertaking QI activities and always looking to improve how we do things. Past examples over the last couple of years have been obtaining competitive funding for Roald Dahl Transition nurse, producing sleep packs, arranging EEG meetings, mental health packs, behaviour management packs, service introduction booklet, clinical summary sheets, patient and parent feedback questionnaires, patient newsletter and participating in Epilepsy12 audit. Our current QI projects are around establishing transition links with adult neurology services, establishing links with local psychology services and exploring how we can start doing MRI with sedation within the hospital.
We have a local patient group run by families whose children have epilepsy. As a way of getting feedback for the last few years we have done feedback questionnaire on Survey Monkey and Google Forms to get their opinion on the service and future areas of improvements. We have created newsletters to keep families updated on our improvement work and hope to be able to do this a few times a year. We would like to establish a patient working group but this has been difficult to achieve given the limited time and resources and therefore have used the feedback questionnaires and newsletter as a way of communication.
We have a few ideas and would appreciate any mentoring one achieving our current quality improvement goals. For our patient group there are a lot of patients with underlying mental health/psychological health needs and we would like to explore ways of screening for these and also pathways to provide appropriate support within the resources we have within the local NHS services and also the voluntary sector. CAMHS referrals are a minimum of a 12m wait at present.
Project planning
Before we participated in the EQIP, we had already begun collating resources to create mental health resource packs, including signposting their patients to local support services. Our ESN has been working with a member of the CAMHS team who is volunteering their time to offer one to one supervision sessions and providing some specific advice for the patients the team are particularly concerned about.
We plan to focus their project on screening tools because there is currently an inefficient process in place. The team have access to discuss their project with a clinical psychologist that works within the one of the local voluntary services. We have sourced one method of screening that uses a well-being index tool which is recommended by the W.H.O. and one that is uses a child outcome rating scale recommended by the local mental health services team.
We plan to begin engaging CYP with eight children that are age 11 to 17. The CYP are in year 10, year 11 and first year of college. Eight of the young people and one parent will be attending six sessions once a week based on managing and understanding emotions. The goal is to produce a booklet together with children and young people and test the preferred method of screening tools out of the two that will be used during the sessions.
Tests, changes and what was learned in the process
November 2022
- The weekly sessions- block of 6. MH screening tool before and after
- Managing & understanding emotions booklet as f/u
- Have access to discuss our project with a clinical psychologist that works in CAMHS and a consultant clinical psychologist that runs a local voluntary charity. The charity is PHEW who supports families with children with physical health difficulties that are causing distress as well as helping children who experience emotional difficulties.
Patient and parent engagement
- Mainly Menti and FTF at the group sessions.
- Parent and child anxiety group with a consultant clinical psychologist.
- Asked if face to face or Teams, what triggers their emotions- upset/ anxiety/ anger.
- Looking to engage with the HOPE group, a parent/ carer and child support group for children and families in Tameside who have a diagnosis of epilepsy.
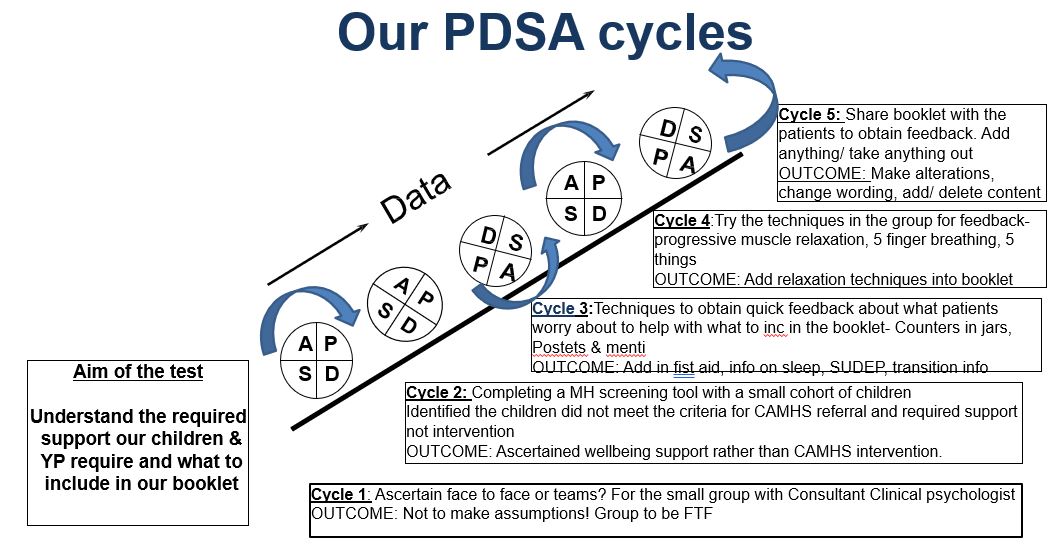
We have already begun acknowledging lessons learnt based on assumptions made that the children and young people would choose to attend sessions virtually (making it easier for the team), however, the response was the opposite where they unanimously fedback they would prefer face to face which came as a surprise to the team.
Next steps
Start the booklet on understanding and managing emotions based on the 6 week group sessions. Use some resources from CAMHS & PHEW.
January /March 2023
- Project hasn’t changed but will possibly be the addition of social stories as a result of feedback and support from CAMHS
- Small patient group over 4 weeks- obtained feedback from the MH Screening tool. Showed them two and they liked the one we liked as a team. Asked if they would like the group FTF or virtual. Obtained what triggers their emotions- upset, anger, anxiety via Mentimeter.
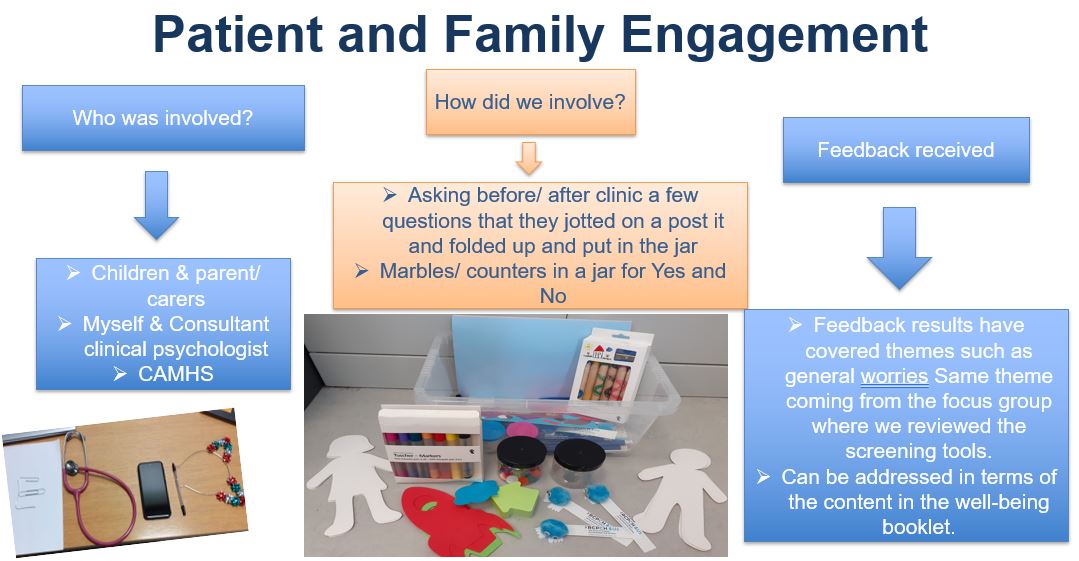
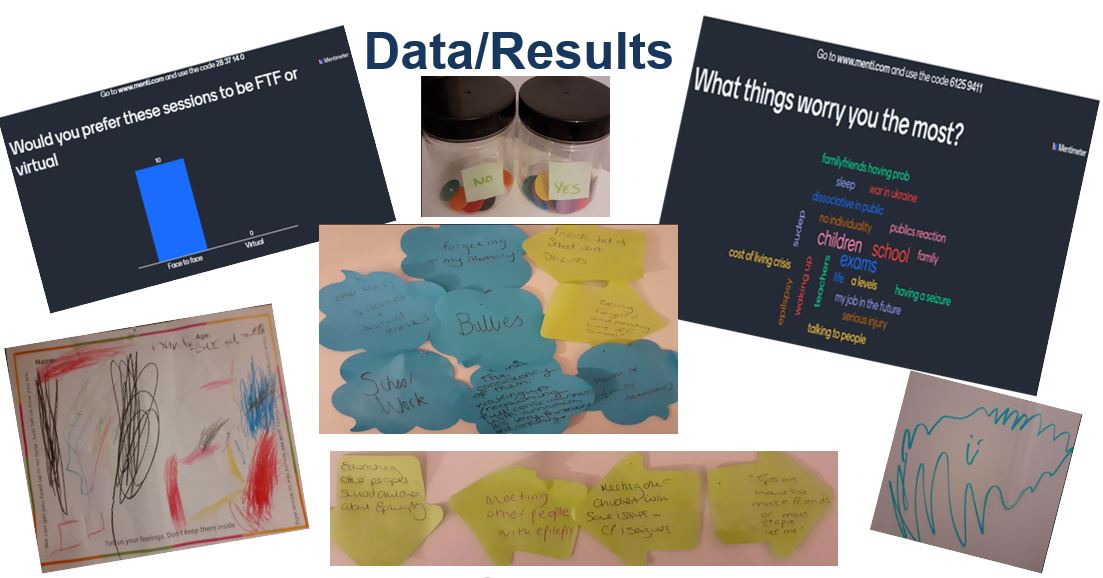
- We have been collating patient and family feedback using Mentimeter and postit note displays.
We received a box of patient engagement materials that that we won during the EQIP Christmas quiz and have been using the materials in clinic. One patient who needs specialist provision was unable to write on the post it notes but was able to draw a picture from the materials in the box. - We are now with the stage of their project of completing their driver diagram and will now begin populating their presentation slides and keep adding to it.
- We are also in the process of creating the well-being pack from the research and been provided with resources and advice from the CAMHS consultant, clinical psychologist that included techniques such as breathing exercises and progressive muscle relaxation.
- We have engaged one or two children and young people to help with providing input into the well-being pack including the clinical psychologist agreeing to review the content before its final draft.
- Additionally, the team have collated feedback from patients on their worries about tests and investigations, having blood tests, having scans. This will result in us creating a social story in collaboration with the clinical psychologist, to help prepare children and young people in terms of coming into hospital for test and investigations using visual aids to present the story along the way.
- Post it notes when children/ YP attend clinic
- Counters in jars
Other assumptions made:
- Small group of children were in High school, experiencing anxiety and awaiting CAMHS. Thought the YP would score low on the MH screening tool (below 13 indicates poor wellbeing) and indication for testing for depression under ICD-10. None of the children at the group scored lower than 13 which highlighted that this could be managed with the wellbeing booklet as ‘early intervention’ whilst awaiting CAMHS or accessing 3rd sector
- We thought feedback about what triggers emotions would be mainly about having seizures/ uncertainty around when next seizure would be. Comments mainly around general worries, feeling safe/ people knowing what to do, parental over protection, meeting other people with epilepsy. This highlighted the booklet could be positive in relation to an action plan and recognizing emotions/ behaviour and strategies to help.
- A lot of feedback around parent/ family/ friends awareness and updates
Next steps
- Continue to collect more data/ feedback from the C& YP
- Begin inputting information in to the presentation
- Start to put together all the information collated and trialled into the booklet
- Bloods, EEG & MRI Scan social stories
- Update driver diagram
- Take pictures of the post it notes
- Link in with the HOPE parent/ children support group. The group took a hit following covid as they were not meeting FTF for such a long time so numbers are low on the monthly meeting. Re launching it which will help in relation to feedback about meeting others with epilepsy and also parental anxiety/ parental overprotection
Results
November 2022
- We asked the children/ YP and their parent what worries them the most (via Mentimeter interactive voting online platform). We thought it would mainly be about anxiety around having a seizure. Big mix really, quite a lot about school (teachers, a levels, exams, a levels, job in the future) bullying, also SUDEP (injuries, sleep, waking up).
- Which mental health screening tool.
- Mental health screening school with the small group before and after the group before we start doing it on a bigger scale.
January/March 2023
- In relation to the screening tool, we thought the children would score worse than they did. None of the children/ YP that completed it scored below 13 (we thought they would). Below 13 indicates poor wellbeing and is an indication for testing for depression under ICD-10. Positive in relation to not requiring CAMHS referral and possibly managing with the understanding and managing emotions work. **Early intervention23.
- Results from the screening tools were not as expected. Did not meet criteria for CAMHS referral/ assessment
- Indicated 3rd sector information & signposting not CAMHS referral.
- Reinforced the need for a wellbeing booklet- understanding & managing emotions.
- Reinforced early intervention before progressing.
April/May 2023
- Majority of children/ YP required support rather than CAMHS intervention
- A lot of general worries- school, friendships & exams
- Patients/ YP worry most about school, safety, investigations, and transition related issues such as exams, college, how to deal with parents
- Parents worry most about SUDEP, after school
- Parents need help and support about getting a healthy balance with encouraging independence whilst ensuring children’s/ YP safety
- A lot of children fed back that they would like to meet other children with epilepsy
- Helped us ascertain what children/ YP would like including in the wellbeing booklet
- Confirmed that children/ YP did need support in relation to their wellbeing
Lessons learnt
- The importance of our monthly epilepsy team meetings!
- The importance of both child/ YP and parent/ carer voices/ feedback
- Majority of our caseload can benefit from adequate signposting and early intervention rather than a CAMHS referral
- Trying different techniques such as QR codes and menti meter
- Changed how we interact and engage with children/ YP.
Not making assumptions!! - Now have a clearer plan, process and support for children/ YP
- Putting into place the feedback received for children & YP to improve their wellbeing and QOL
- Lots of ideas for our new transition service
- As a result- working with CAMHS to devise social stories for bloods, MRI scan and EEG
- Re advertising the HOPE group
Challenges
- Poor uptake to the group due to unwell/ seizures as winter Dec/ Jan when started the group.
- Team is motivated but limited time. Often arrange meetings but cancelled due to A/L, workload, consultant hotweeks/on call
- Face to face Group was harder to coordinate in relation to room availability and size
- Planned to invite 10 children/YP and their parents. As it was face to face could only invite a max of x5 children with a parent/ carer due to room size and space (Could of invited more virtually)
- 6 week parent/ YP group with Consultant clinical psychologist ended up over 4 weeks due to arranging it for Dec/ Jan. As it was during the height of the winter period there was parent/ patient illness/ admissions resulting in x2 session having to be cancelled
- Clinical psychologist from CAMHS who the team has 3 weekly supervision with handed notice in and leaving with no allocated replacement.
- This project has been undertaken at a time of significant staff change within the team
- Impact of nursing and doctor strikes, strep surge on staff & the service
Successes
- A clinical psychologist from CAMHS and a consultant clinical psychologist who works with a charity (PHEW) have both been keen to provide some input in relation to supervision sessions and a joint group on understanding and managing emotions.
- The children attending are getting more confident to engage as the sessions have gone on.
- No clinical psychology in the team but as a result of reaching out, sparked the idea and managed to secure monthly/ bi monthly supervision. The supervision sessions enabled a clear plan. If triggered high on the screening tool could obtain consent to discuss at supervision, referral in to CAMHS, advice in the interim.
- Established screening tool (WHO) in the small group workshop.
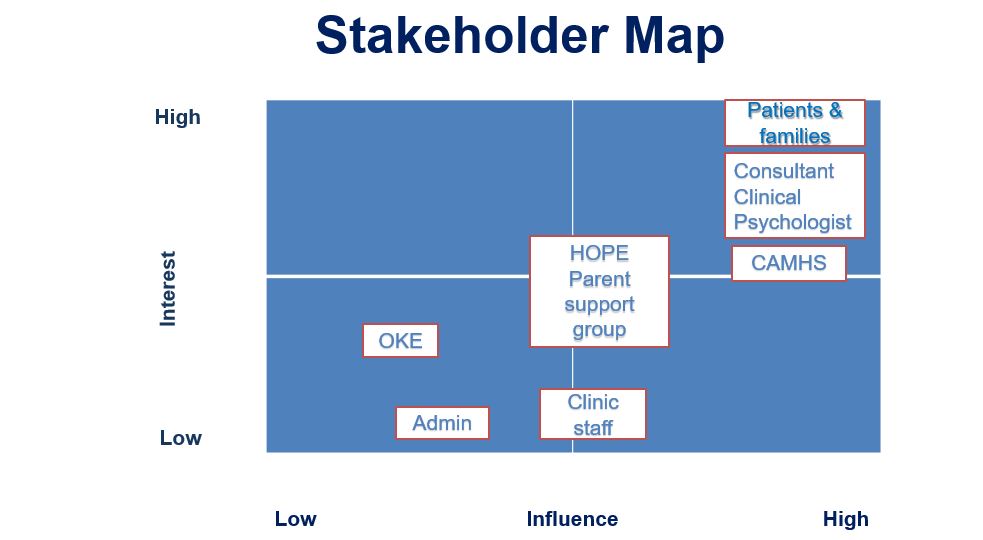
- Stakeholder engagement- Clinical psychologist from CAMHS, assistant clinical psychologist, and Consultant clinical psychologist from the charity PHEW & MH/ substance mis-use nurse
- During the 4 week groups was able to try out the techniques with the YP- breathing exercises (5 finger breathing), 5,4,3,2,1 grounding, progressive muscle relaxation which provided good feedback and will add into the booklet.
- CAMHS Supervision
- Following patient/ carer information/ feedback received- identified worries regarding required tests and investigations (MRI without sedation, EEGs and blood tests). Currently 12-18m wait for an MRI scan without sedation vs 4 weeks without sedation. The wait can lead to heightened patient and prental anxiety. This has led on to discussing with CAMHS and working with an assistant clinical psychologist to develop x3 social stories (blood test, MRI and EEG). With the intention to provide the children and young people on our caseload with information and adequate preparation with the aim to reduce anxieties. Also prevent the need for refusal of investigations.
- Linking in with the HOPE Group (parent/ Child support group)
- Support and patience from EQIP including great lectures and great insight into patient engagement
- Appointing a transition nurse within the team is a positive step in improving this area. The worries highlighted around transition can be addressed
- Understanding that parents and children/ YP often have very different worries. Often parental worries are worse and need addressing to ensure it doesn’t impact the child/ YP.
Next steps
- Changing our practice and potentially other teams practice by sharing
- Once in post can reinstate work with CAMHS- Monthly/ bi monthly supervision where we can discuss cases and where best to signpost
- Set up a parent/ carer event with CAMHS/ OKE about managing parents/ carers emotions/ worries/ fears
- Transition & teenage groups to meet peers with epilepsy and cover worries that were addressed around school, friendships, exams, college and employment
- With CAMHS devising social stories to help with worries around blood tests, EEGS and MRIS
Locally
- Share at the HOPE group (monthly child/ YP & parent/ carer support group)
- Local specialty/ governance/ team meeting
- Share our experience- Possibly at the NWEIG
- Consider implementing screening tool to highlight MH concerns at clinic
Team presentations and project posters
Tameside and Glossop Integrated Care NHS Trust team presentations and project posters
Download to view Tameside & Glossop team presentation slides and poster
Team presentation slides (8.4MB) Team project poster (1.3MB pdf)