
Medway NHS Foundation Trust
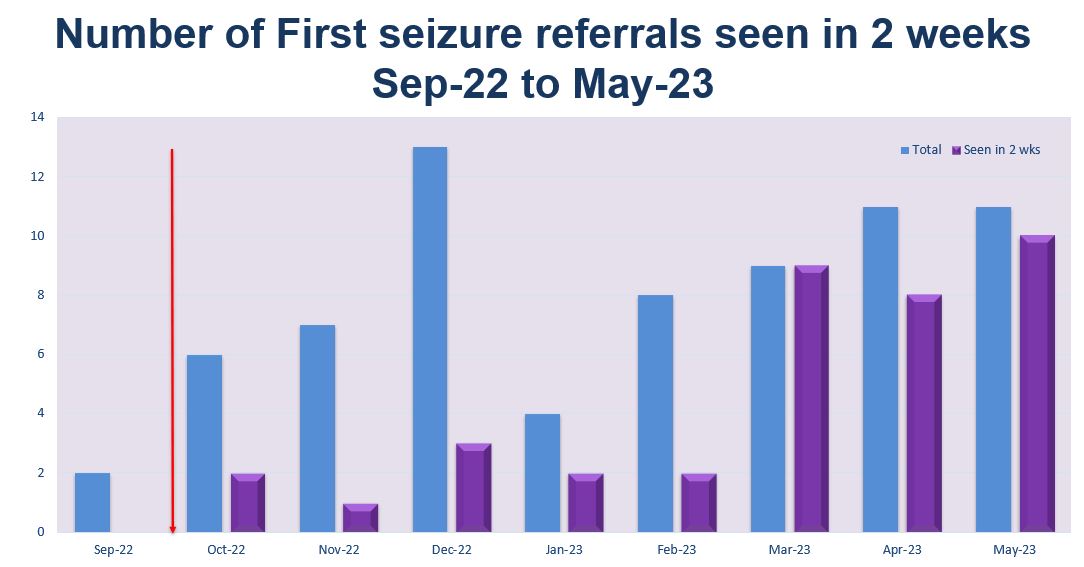
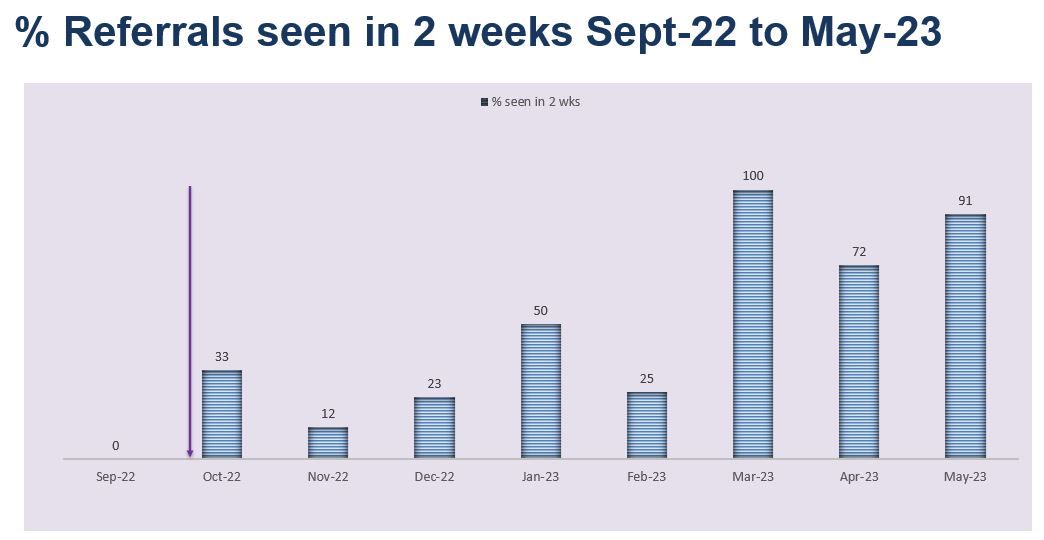
60% of first seizure referrals are seen within 2 weeks by May 2023

Project aim
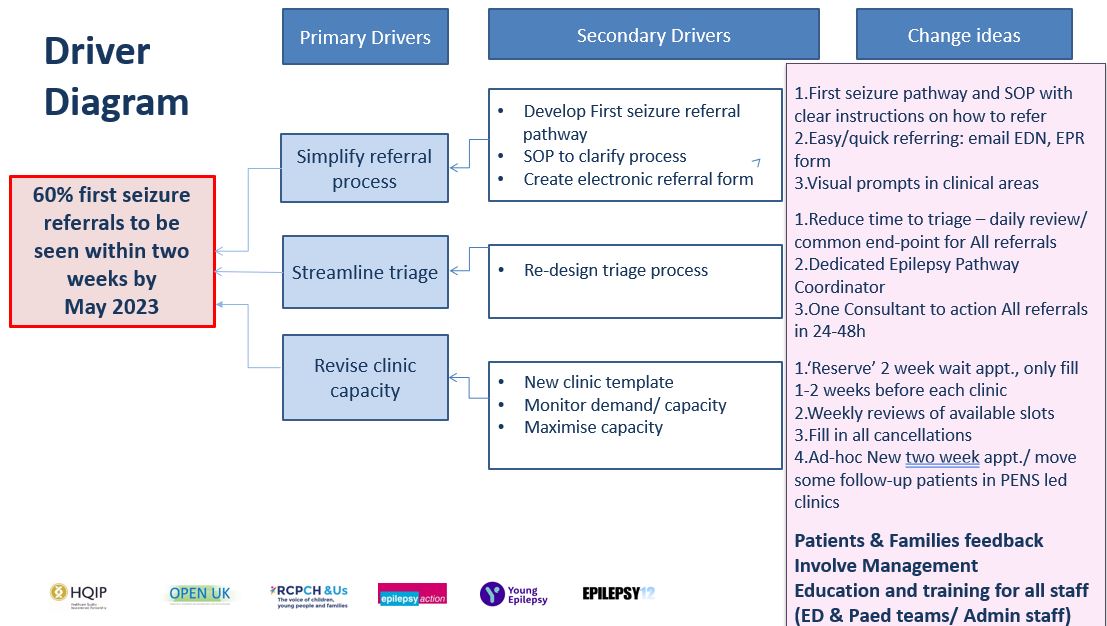
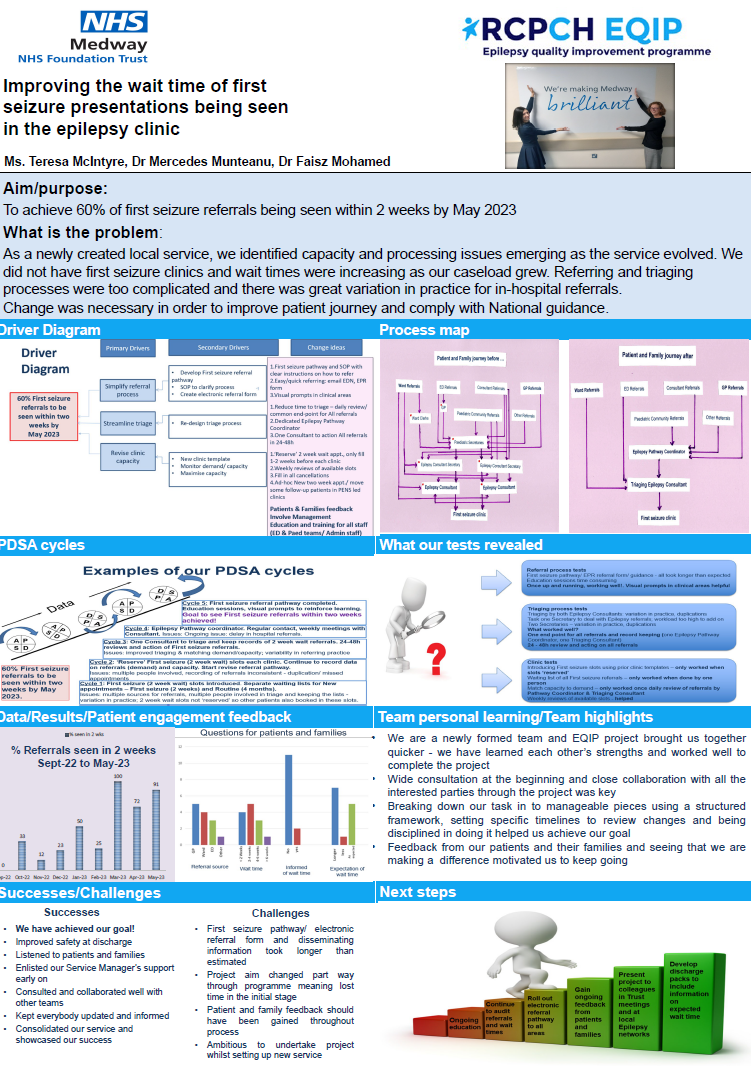
60% of first seizure referrals are seen within 2 weeks by May 2023.
Background
Our team consists of 2 consultant paediatricians with a specialist interest in epilepsy and a clinical nurse specialist appointed in April 2022, thereby making us a new service. Many children we care for have joint care with Evelina London and King’s College Hospitals as well as community input. Although we are in the process of creating a database illustrating our caseload, we estimate the number of children who could fall under our care to be approximately 400 – 500.
We are looking locally (and informally) at the number of families who live in the geographical region of Swale to see if the distance from the hospital and public transport limitations are factors which contribute to some families not attending their clinic appointments. If the evidence suggests these are factors, we hope to implement monthly clinics in the Swale region.
We would implement a referral pathway into our service, initially focusing on A&E presentations and ward attenders but, when the process is deemed robust, we would roll ot a pathway for GP practices.
Project planning
We would like to develop a referral pathway for children and young people with first seizure presentation. The referral will be two-fold. One pathway will be in an electronic format for referrals from the Children’s Emergency Department, whilst the other would be a paper format (with a master copy available on a shared database) for referrals from the Children’s Ward and Children’s Assessment Unit.
Our idea for this project came from our experience of receiving inappropriate or incomplete referrals from members of the hospital team which either did not have sufficient information on the referral or were not suitable to be seen in our first seizure clinic (for example typical febrile seizures). We felt this initial process was so important in order to identify what our best practice should look like, and therefore decided this was the area we would most like to improve.

Tests, changes and what was learned in the process
November 2022
- Following the development of the electronic referral pathway, we will trial this as soon as we can and gain feedback from the team members using this method of referral. We want to ensure the pathway is user friendly and has all the relevant information on it.
- We will pass both the electronic and paper versions through our governance department for review, comments and questions from team members.
- We will present our proposal to our Consultant body in December and ask for comments and questions from this meeting which may shape our progress moving forward.
- We will be carrying out teaching sessions with all staff to go through the referral forms and include the reason why certain criteria are on the form (for example the rationale for carrying out an ECG)
- We will audit the referrals that come to us via the new system and continually to do so in order to see if the form needs to be changed in any way to ensure appropriate referrals are sent to our service.
- We are working on developing a linkage process where the EPR system generates a generic e-mail when an electronic referral is entered onto the system then automatically sent to the team. We plan to focus on improving the inhouse referral pathways first, before working on improving GP referrals.
Patient engagement
We feel there is a great need to implement a robust referral pathway in order to ensure all children and young people experiencing a first seizure, are seen in a timely manner in an appropriate manner.
Next steps
- Create a generic email address for the Epilepsy team which will be linked to the electronic referral pathway thereby generating an email to key designated staff once the referral is submitted.
- Meeting with the EPR (Electronic Patients Records) team this week to devise an electronic referral pathway which we hope to roll out before Christmas.
- Teaching of the ED staff in relation to this pathway.
January 2023
Following our first 1:1 meeting, we have decided to narrow down our project looking at the epilepsy referral pathway for use in hospital. Initially the pathway will be used in Children’s Emergency Department and will then be rolled out to the rest of the Paediatric services.
Our idea for this project came from our experience of receiving inappropriate or incomplete referrals from members of the hospital team which either did not have sufficient information on the referral or were not suitable to be seen in our first seizure clinic (for example typical febrile seizures). We felt this initial process was so important in order to identify what our best practice should look like, and therefore decided this was the area we would most like to improve.
We have now devised an electronic referral pathway which will be shared with the paediatric teams across the Trust. Once feedback is gained and comments taken on board, it will go live by the end of February following submission to governance. Teaching will occur on a weekly basis for all those who will use the pathway in ED and on the ward, and we plan to re-evaluate the referral process once it has been in place for one month. The re-evaluation will be ongoing and changes made where necessary.
Patient engagement
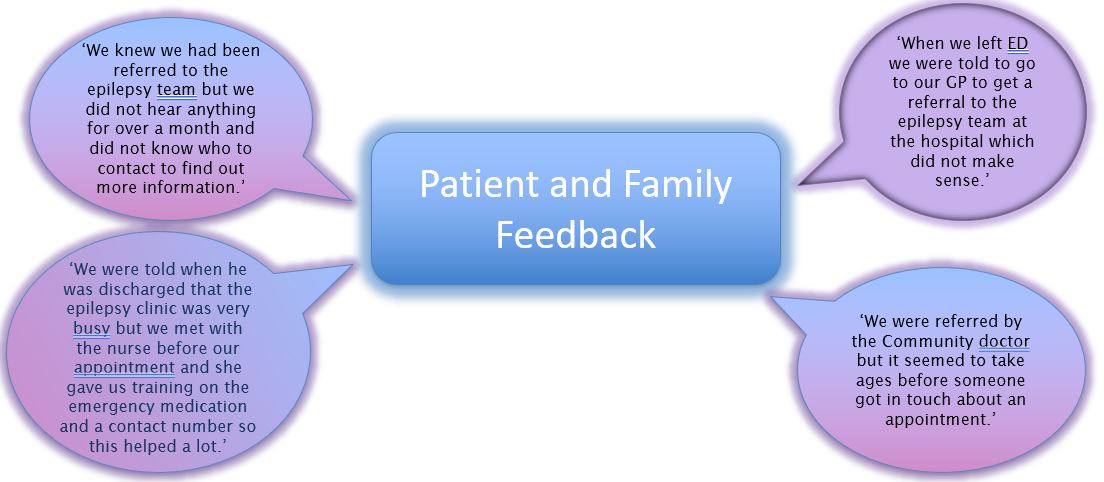
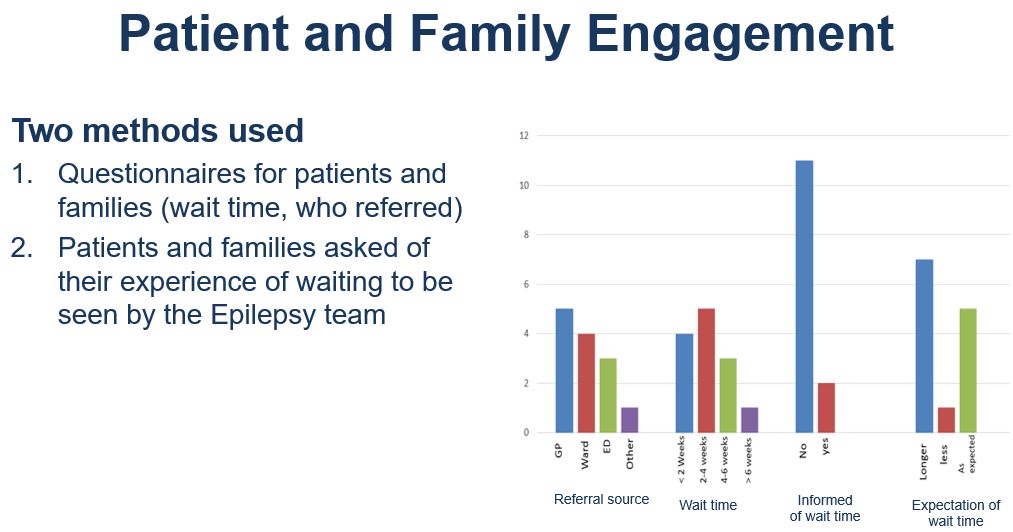
We have given out questionnaires to a small number of families and young people asking for their experience of the referral process. We are waiting for some more replies before we can ascertain to what extent the referral process is working currently, and also to see how we can improve. The idea of the questionnaire is to give a baseline as to where we are, on average, with our referral timeframe at the moment. This will also give us an indication of the ‘journey’ through the referral pathway for families and children and young people.
Next steps:
- Follow up on the generic email address for the Epilepsy team which will be linked to the electronic referral pathway thereby generating an email to key designated staff once the referral is submitted.
- Gaining feedback on our referral pathway.
- Re-evaluate regularly and make changes as needed.
- Teaching of the ED and Ward staff in relation to this pathway.
March 2023
Our project aim has changed slightly from the beginning of the programme in that we hoped to develop a paper version of the electronic referral form also. Although this is something we still aim to do, we decided to concentrate on one aim as we feel this is more achievable and will be transferable when the Trust moves solely to electronic record keeping.
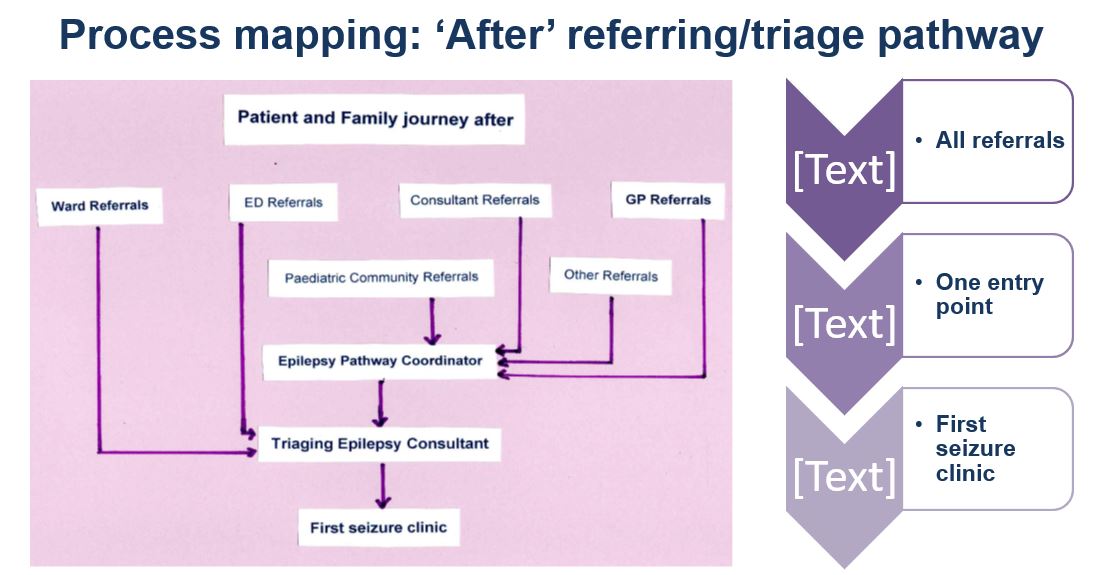
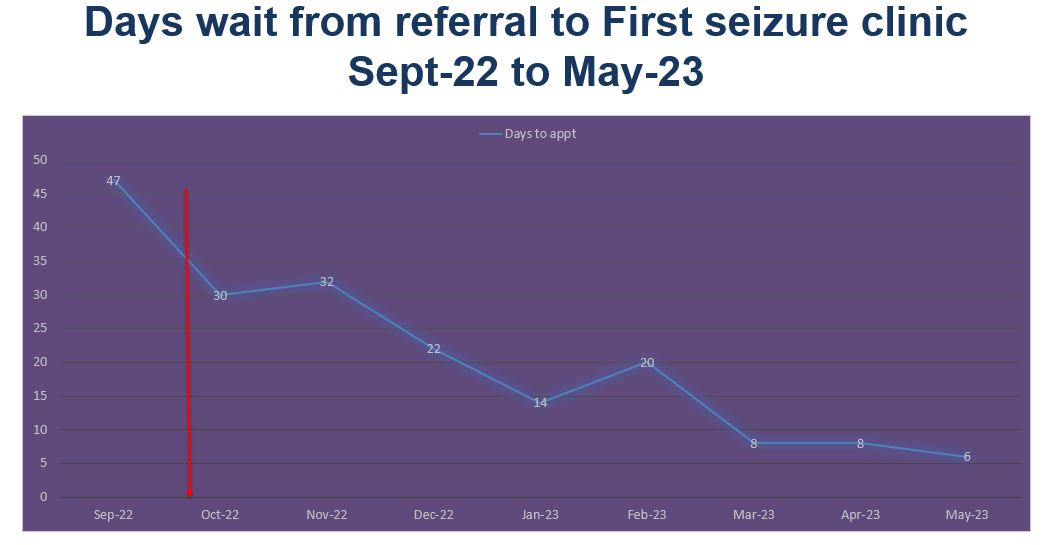
We reviewed one month of data from children and young people seen in our clinics, and easily identified that the current referral process was inadequate and inconsistent. We did not meet National Guidelines (i.e. those presenting with a first seizure should be seen in clinic within a two week timeframe). By completing the newly constructed referral pathway, a message will be generated to our team on the day the referral is made. We can then enlist the help of our newly appointed pathway coordinator to book the patient into the first available ‘first seizure’ slot. This initial step is essential as it sets the tone for the rest of the patient journey.
The form has been designed and has been sent to the Electronic Patient Records team for tier input in to how it can be put on the Trust’s electronic records system. We have trailed inputting data on the form in the office environment only, and have had to make changes on three occasions so far. One of the changes included not using the generic email address we created to get notifications of new referrals, but instead, using a patient list that would be populated with any new referral data. We were unaware of a system such as this, but with guidance and input from the EPR team, this makes sense and makes it more user-friendly for all. We hope to have the form ready to use within 4 weeks.
We have teaching and feedback sessions lined up with the team in ED whereby we will talk through the form and work through an example of how it will be used, but we will act on their experience and comments as they will be the ones using the form in the first instance. By doing this, we hope to achieve a user-friendly form that can be used across all specialties when electronic records are in place across the Trust.
The form has been through our Governance team and has been passed following comments made by our colleagues within the Trust.
We obtained feedback in clinic from families referred to us in recent months. We focused on the method of the initial referral (i.e. ED, GP) and the length of time it took for us to see them from referral to appointment. Although we could see an improvement in the wait times, we still identified the need to improve upon our times as we were not meeting National Guidelines. Something else we looked at was the expectation the family had in terms of wait times to see a Consultant, as some of the information given by other health care professionals was inaccurate and not in line with the service we offer.
We plan to continue to audit the referrals that come to us via the new system and make any changes necessary to ensure it is fit for purpose.
Patient engagement
We continue to see the benefit of a bespoke first seizure referral pathway to benefit all those with a first seizure presentation.
Having spoken to families now under our care, we realise there is a need to streamline our referral process in order to improve the patient journey and also meet National Guidelines.
Auditing family responses regarding appointment wait times, and looking at sources of the referrals in conjunction with this, has again highlighted the need for a standardized referral pathway that can be used by all health care professionals wishing to refer to our service in the future.
Next steps
- Completing our presentation storyboard.
- Collating all the data we have so far collected.
- Looking at the poster template to ensure we are ready for questions during the May drop in sessions.
- Teaching of the ED staff in relation to this pathway.
Results
November 2022
Auditing our referrals once the system is in place will tell us if the pathway is a useful tool to use.
January 2023
Awaiting more data from questionnaires recently given out.
March 2023
- Wait for the final version of the electronic form to be presented and review it to ensure it is user friendly.
- Look at the wait time from referral to appointment time when the new system is in place. This will be done by looking at our own data and also getting feedback from families in the same way we are currently collecting our data.
- Gain ongoing feedback from those using the referral form to ensure it meets all expectations.
- Ensure the use of ‘patient lists’ to monitor number of referrals to our service, is an easy system to use that captures all relevant data.
Referral process tests
- First seizure pathway/ EPR referral form/ guidance – all took longer than expected
- Education sessions time consuming
- Once up and running, working well!
Visual prompts in clinical areas helpful
Triaging process tests
- Triaging by both Epilepsy Consultants – variation in practice, duplications
- One Secretary to deal with Epilepsy referrals – workload too high
- Two Secretaries – variation in practice, duplications
What worked well?
- One end point for all referrals and record keeping (one Epilepsy Pathway Coordinator, one Triaging Consultant)
24-48h review and acting on all referrals
Clinic tests
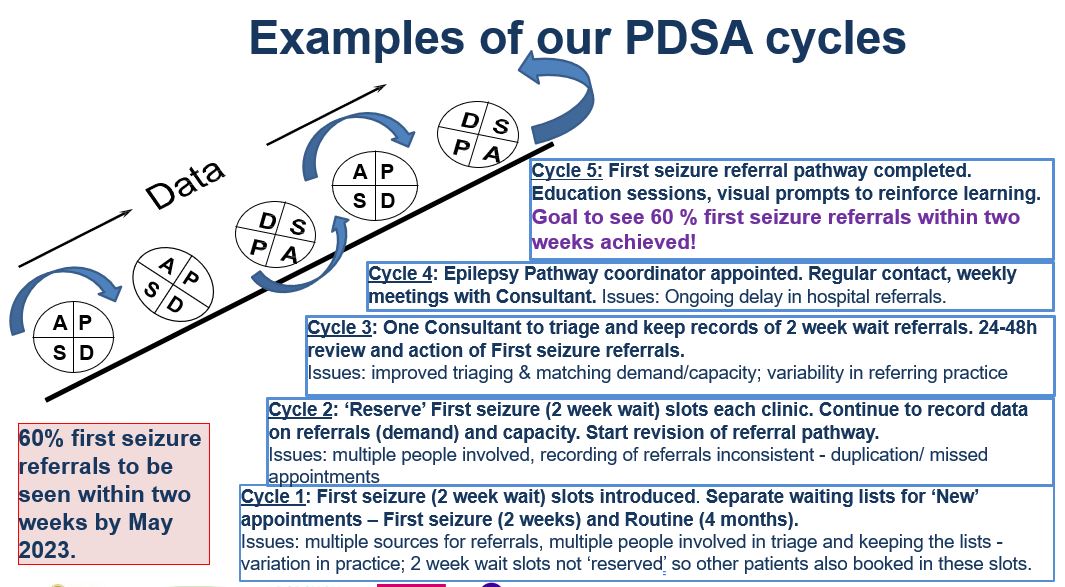
- Introducing First seizure slots using prior clinic templates – only worked when
slots ‘reserved’ - Waiting list of all First seizure referrals – only worked when done by one
person - Match capacity to demand – only worked once daily review of referrals by
- Pathway Coordinator & Triaging Consultant
- Weekly reviews of available slots – helped
May 2023
- We are a newly formed team; the EQIP project brought us together quicker – we have learned each other’s strengths and worked well to complete the project
- Wide consultation at the beginning and close collaboration with all the interested parties through the project was key
- Breaking down our task in to manageable pieces using a structured framework, setting specific timelines to review changes and being disciplined in doing it helped us achieve our goal
- Feedback from our patients and their families and seeing that we are making a difference motivated us to keep going
Challenges
- Receiving inappropriate or incomplete referrals from members of the hospital team which either did not provide sufficient patient information on the referral or patients that were not suitable to be seen in the first seizure clinic (for example typical febrile seizures).
- Unaware of actual caseload numbers due to systems that are incompatible with each other across sites.
- Receiving random emails via ED to see patients without following any clear referral processes and providing inaccurate or missing information.
- Half of the hospital children’s ED use electronic records which is recorded on the Trust EPR records, however, inpatient wards and assessment units use paper referrals.
- Receiving referrals from three separate depts within the Trust which is difficult to keep track of the referrals received by their service.
- We were unsure which pathway to focus on due the team discovering the low number of referrals received from the ED dept.
- Once the new pathway is in place we anticipate that appointments slots may not meet demand.
- There was no baseline data available to capture the number of GP or internal ward referrals received by the service.
- Lack of clinic slots available therefore difficult to meet the two week wait target all the time.
- Time consuming process currently looking at all referrals individually and with different information on it. The amount of information given can vary hugely between one referrer and the next and we often spend time going through clinical records to get more information about the child or young person being referred to us.
- Annual leave and covering during industrial action has led to cancellation of some clinics therefore setting us Our current challenge has been that we have not been able to meet as a full team due to annual leave and sickness, however we will endeavor to meet regularly to ensure we are all aware of the progress of the project, and to ensure all members of the team are involved equally.
- Currently we are trying to find time to sit down and populate our storyboard as we are seldom all together except when in clinic. We have a lot of information from our project so far, (we think) but taking time to put it together in an ordered way is proving a challenge, however we remain a small but motivated team, keen to highlight the work being carried out in our hospital.
Successes
- Referral pathway written and ready for implementation. Other members of the Paediatric team now aware of the plan with regards to new referral and are therefore adopting more uniform approaches in referring to our team.
- Appointment of pathway coordinator dedicated to the epilepsy service is a bonus and will provide consistency when it comes to our booking methods. Also, this person can keep contemporaneous referral information and update our current databases so as to ensure all those referred to us are monitored and not lost to follow up.
- We have achieved our goal!
- Improved safety at discharge
- Listened to our patients and their families
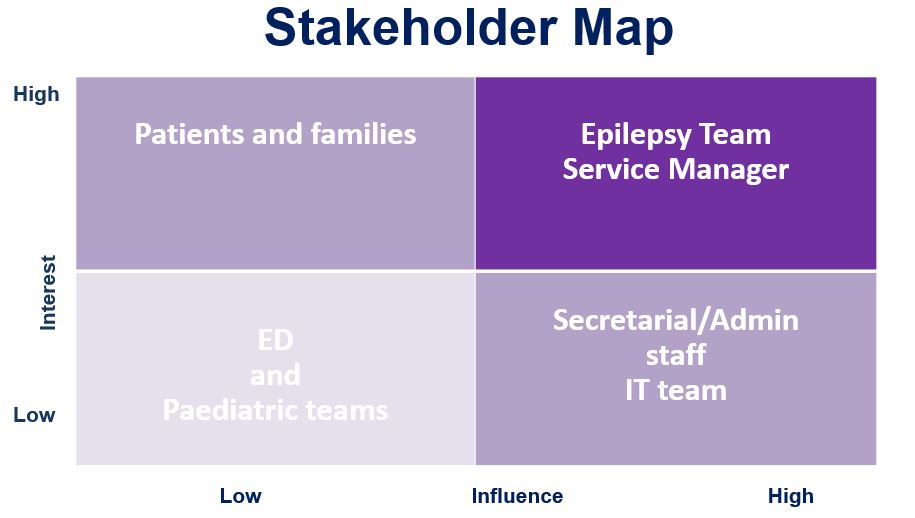
- Enlisted our Service Manager’s support early on
- Consulted and collaborated well with other teams
- Kept everybody updated and informed
- Consolidated our service and showcased our success within the Trust
Next steps
- Include information on expected wait time in discharge packs as this was something highlighted as lacking in our questionnaire response
- Gain ongoing feedback from patients and families
- Ongoing education
- Roll out electronic referral pathway to all areas when available
- Continue to audit our referrals and wait times
- Present project to our colleagues in Trust meetings and at local Epilepsy networks
Medway NHS Foundation Trust team presentations and project posters
Download to view Medway team presentation slides and poster
Team presentation slides (6.9MB) Team project poster (1.3MB pdf)